Abstract
The stomatognathic system is extremely important for the body, as it integrates functions such as chewing and swallowing. Furthermore, according to recent studies, there is a relationship between this system and brain safety, affecting areas of the hippocampus and cortex, which suggests that the loss of stomatognathic efficiency may contribute to cognitive decline. Thus, changes in the occlusal plane gain prominence, considering that they affect the chewing cycle. Therefore, the objective of this study is to correlate occlusal pathologies (overbite, temporomandibular dysfunction and absence of dental elements) and functions of the stomatognathic and cervical muscles through an electromyographic analysis of these individuals. The muscles were evaluated at the Dentistry Clinic at Faculdade Arnaldo in two different moments: before the clinical evaluation and 15 minutes after the initial assessment, in order to observe short-term changes in muscle activation patterns. The objective was to investigate the electromyographic behavior of masticatory and cervical muscles in a patient with temporomandibular dysfunction.
Highlights
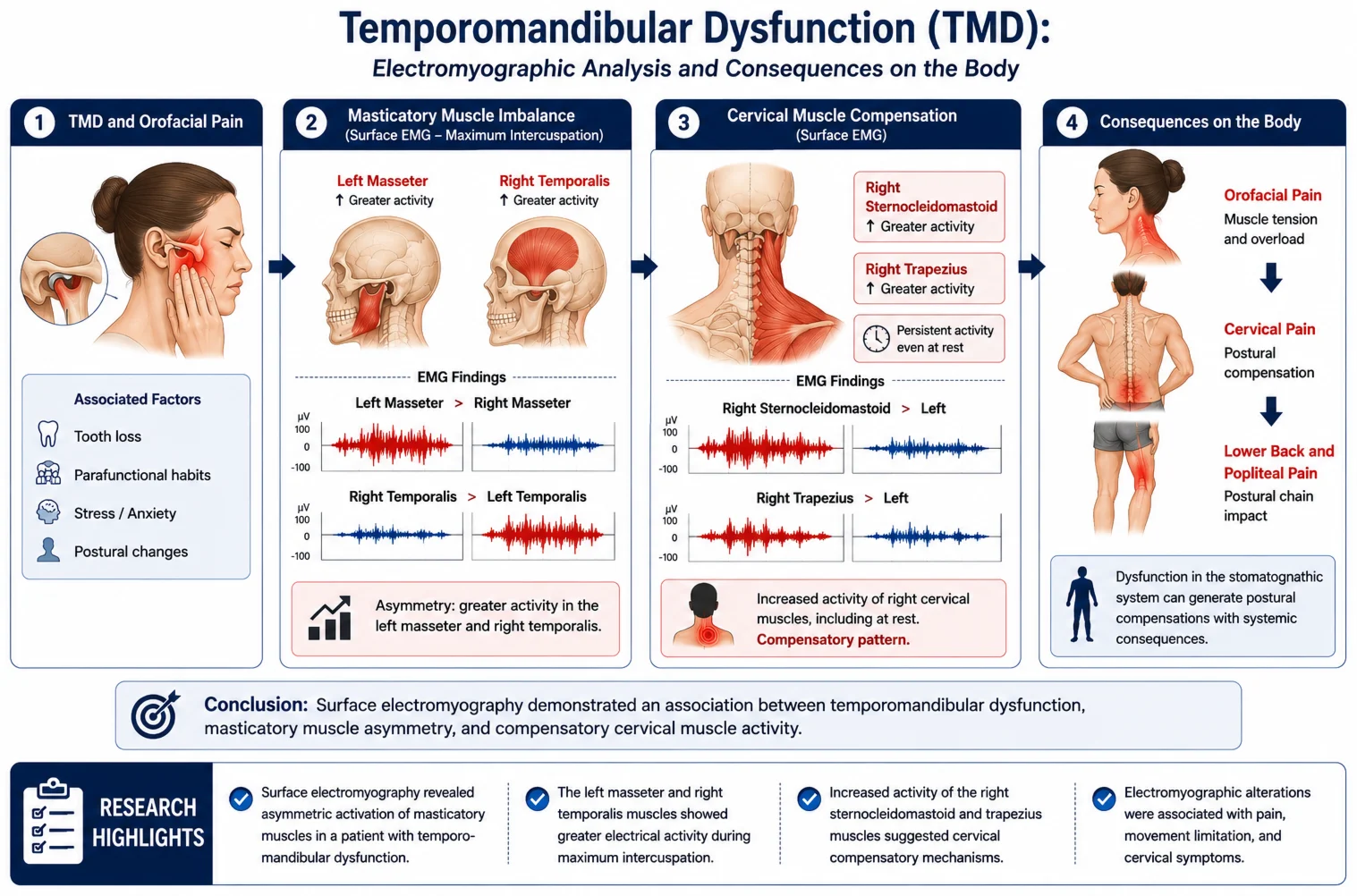
- Surface electromyography revealed asymmetric activation of masticatory muscles in a patient with temporomandibular dysfunction.
- The left masseter and right temporalis muscles showed greater electrical activity during maximum intercuspation.
- Increased activity of the right sternocleidomastoid and trapezius muscles suggested cervical compensatory mechanisms
- Electromyographic alterations were associated with pain, movement limitation, and cervical symptoms.
1. Introduction
Temporomandibular dysfunction (TMD) is a disorder between the temporomandibular joint and the chewing muscles, and is associated with symptoms such as: pain, limited movement and muscle stress. This process is coordinated by neural pathways and synaptic connections established and controlled by the cerebral cortex, playing an important role in the stomatognathic system. Furthermore, studies point to the importance of muscular activity for brain functions, as well as for the prevention of cognitive decline [1], [2]. The main hypothesis is that one, temporomandibular dysfunction, [3] would affect muscular harmony, leading to decreased activity and consequently a reduction in cerebral blood supply, [4], [5] thus resulting in a cascade effect, with a systemic effect on the body [6]. The absence of muscular harmony may lead to chewing and nutritional alterations. Experimental and clinical studies suggest that reduced masticatory stimulation may be associated with alterations in hippocampal neuroplasticity, cerebral blood flow, memory processing, and cortical activation, which could contribute to cognitive decline and neurodegenerative processes.
In particular, current studies reveal that the peripheral deafferentations of stomatognathic systems may be projected globally into the central nervous system (CNS) and become an associated critical factor in triggering and aggravating neurodegenerative diseases [7-9]. Another hypothesis is that this disorder would cause changes in the central pattern generator, which is essential for the well-being of the cerebral cortex. A study demonstrated that participants with severe cognitive impairments exhibited fewer occluding pairs and a smaller active mouth opening. These participants experienced neuromuscular dissonance caused by temporomandibular disorder (TMD). The deafferentation and alterations in the teeth and masticatory apparatus may result in brain damage due to altered cerebral circulation and dysfunctional homeostasis [7], [9].
From this perspective, this study came up with the idea of evaluating how a muscular dysfunction can affect the chewing muscles, which would lead to a reduction in the efficiency of muscular activity with serious systemic consequences. [5] Temporomandibular dysfunction may be associated with psychosocial factors, parafunctional habits, genetics, stress and anxiety, postural changes, jaw trauma, excessive mouth opening, and may also be aggravated by pre-existing diseases or occlusal interferences [9], [10] factors that contribute to this muscle stress, [13] due to longer muscle contraction during chewing [14], [15]. In other words, it can influence the pattern of muscular coordination during the act of chewing, reducing its intensity and prolonging muscular activity, which can cause painful symptoms [16].
Complaints of difficulty chewing are common in dental offices and may be related to temporomandibular disorders, causing dental trauma such as: cracks, teeth wear, cervical lesions. Therefore, realizing the possible correlation between joint dysfunction and disharmony of the stomatognathic muscles, it could lead to damage to brain areas such as the hippocampus. There is a need to evaluate muscular conditions in the face of TMD, which can be explained by: muscular hyperactivity as a compensatory form for joint-tooth-muscular disorder, clenching, morphological changes in the joint region and temporomandibular dysfunction [16].
Complaints of difficulty chewing are common in dental offices and may be related to temporomandibular disorders, causing dental trauma such as: cracks, teeth wear, cervical lesions. Therefore, realizing the possible correlation between joint dysfunction and disharmony of the stomatognathic muscles, it could lead to damage to brain areas such as the hippocampus. There is a need to evaluate muscular conditions in the face of TMD, which can be explained by: muscular hyperactivity as a compensatory form for joint-tooth-muscular disorder, clenching, morphological changes in the joint region and temporomandibular dysfunction [16].
Thus, the objective is to analyze the impact of temporomandibular dysfunction, so that appropriate measures and prevention can be applied in the dental field. With this, the strength of the chewing muscles will be analyzed in patients with a dysfunction and control patients in and after individual treatment for each patient to assess the impact on the chewing cycle, the muscle and the body.
2. Case report
Patient A.C., 29 years old, female, came to the Temporomandibular Dysfunction Clinic at Faculdade Arnaldo, in Belo Horizonte-MG, complaining of pain during chewing on the left side. During the anamnesis, she complained of headache when she wakes up, frequent pain in the cervical region, pain when opening the mouth and difficulty opening the mouth in the morning after waking up. Regarding habits, it was reported that she sleeps with her hand under her face.
The extraoral clinical examination showed some alterations, namely: 1) Deviation of opening and closing to the right; 2) Creptus on the right side during the opening movement; 3) Medium intensity popping on the right side during the opening movement; 4) Pain during forced movement; 5) Pain during palpation of the right temporal bone; 6) Bilateral volume of the masseter and temporal bone; 7) Bilateral jump at the moment of the middle and end of the movement; 8) Pain on palpation of the left masseter.
The laterality movements (right and left), protrusion, and maximum mouth opening were measured. For maximum mouth opening, the patient was asked to open as maximum as possible without any pain, and performing the interincisal measurement the value obtained was 55mm. The protrusion movement is performed through the patient's occlusion, measuring the distance from the vestibular surface of the lower incisor teeth to the incisal surface of the upper teeth. Then, the patient was instructed to perform the mandibular protrusion movement, obtaining a vertical measurement of 2.5 mm and a horizontal measurement of 1.2mm. During maximum laterality, there was a difficulty in performing the movement on both the right and left sides; on the right, there was a measurement of 4.0 mm and on left, 5 mm.
For pain assessment, a visual analogue scale from 1 to 10 was used, where 1 would be discomfort and 10 would be incapacitating pain, making it difficult to perform the movement proposed by the evaluators. During the assessment, the following were observed: (I) pain on palpation in the left masseter with a score of 7, (II) pain in the right temporal bone with an intensity of 7, (III) pain in the left temporal bone with an intensity of 6, (IV) pain in the right and left trapezius with an intensity of 8, (V) pain in the right sternocleidomastoid with an intensity of 7, (VI) pain in the left sternocleidomastoid with an intensity of 5, (VII) pain in the right and left dorsal region with an intensity of 7, (VIII) pain in the right popliteal region with an intensity of 7.
Regarding the stomatognathic muscles, pain of level 5 was reported in the right masseter during passive movement, and pain of intensity 4 in the right temporal muscle. During forced movement, pain was reported as intensity 6 in the left masseter, and also intensity 6 in the right temporal muscle. Regarding palpation, pain of intensity 7 was reported in the left masseter and intensity 6 in the right temporal muscle. In addition, muscle nodules were observed in the masseter and temporal muscle on both sides. When analysing the lateral movement, it was difficult to perform it on both the right and left sides.
For better understanding of the muscle behaviour, the patient was asked to undergo an electromyographic analysis of the masticatory muscles (right and left masseter; right and left temporal muscle) and cervical muscles (right and left trapezius; right and left sternocleidomastoid).
The equipment used to collect muscle data was an electromyograph, attached to a computer with the aid of Myosystem-Br1 software. Its function is to record the signals obtained and transform them into pulses of action potentials of motor units, leading to a triggering of electromyographic impulses observed on the computer. The equipment model is the Myosystem Br1 P84/DATAHOMINIS Tecnologia® (Uberlândia, MG, Brazil), which has twelve channels, eight for electromyography and four auxiliary channels. In addition, sampling will be done with frequency regulation at 8000 Hz in each channel. All electromyographic recordings were collected during daytime under natural light conditions. The patient remained seated in the Frankfurt plane position near a window throughout the examination. All equipment was connected to a standard 127-V electrical supply. No obvious sources of electromagnetic interference were identified in the recording environment.
Furthermore, the electrodes that were attached to the channels of the myographic collection equipment have two parallel metal plates measuring 10 mm in length and 1 mm in width, spaced 10 mm apart. A ground electrode was positioned on the glabella region after skin cleansing with 70 % alcohol. Before electrode placement, the skin was cleaned with 70 % alcohol to reduce skin impedance and improve signal quality. Electrode placement followed recommendations from previously published electromyographic studies involving masticatory and cervical muscles. Surface electromyography recordings were obtained bilaterally from all muscles analyzed.
To collect muscle data, prior the skin was prepared by cleaning with and alcohol wipe, then the electrodes were positioned with the aid of micropore tape were placed on the muscle belly parallel to the muscle fibers, follows with the billatery: on the temporal muscle, 2 cm vertically above the zygomatic muscle and 2 cm horizontally anterior to the eye socket, on both sides. To measure the masseter muscle, the electrodes were positioned horizontally 2 cm anterior to the mandibular border and vertically 3 cm above the mandibular border, on the left and right sides. To measure the paravertebral cervical muscles, the electrodes were positioned 5 cm vertically above the sternocleidomastoid muscle and 3 cm above the T1 vertebra, bilaterally. That way, the following were analyzed: electrical activity of the bilateral temporal muscle, bilateral masseter muscle, bilateral cervical muscle, with three electromyographic tests that lasted five seconds with a 30 second interval between each one, taken in the resting position of the jaw and during maximum intercuspation. A five-second recording period was selected because it is commonly used in surface electromyography studies and allows stable signal acquisition while minimizing muscle fatigue. A 30-second interval between recordings was adopted to avoid muscular fatigue and ensure signal reproducibility.
The participant was instructed to sit in a chair, with relaxed shoulders and hands resting on a backrest, with the head positioned at Frankfurt plane parallel to the floor. During the electromyographic measurement, the patient did not receive feedback or recordings of muscle activity, in order not to influence the results. The measurements were taken three times for each: maximum intercuspation and resting position, as well as for the bilateral masticatory muscles and the bilateral neck muscles.
Resting position: the patient was instructed to relax and keep the maxilla and mandible halfopen, without any dental contact between the upper and lower teeth, the measurements were taken bilaterally for the masticatory muscles, with three repetitions and a 30-second interval between each. Similarly, the measurements were taken bilaterally for the neck muscles, with three repetitions and a 30-second interval between each. Maximum intercuspation: the patient was instructed to clench her teeth as hard as possible and maintain the level of muscle contraction. Similarly, bilateral measurements were performed for the masticatory muscles, with three repetitions and a 30-second interval between each, as well as for the neck muscles, with three repetitions and a 30-second interval between each.
During maximum intercuspation of the masticatory muscles, the first session demonstrated greater electrical activity in the masseter muscle on the left side, as well as in the left temporal muscle (Fig. 1), but this session was disregarded due to the discrepancy in the electromyographic pattern of the second and third sessions.
Abbreviations: massd = right masseter muscle; masse = left masseter muscle; tempd = right temporalis muscle; tempe = left temporalis muscle; pesd = right trapezius muscle; pese = left trapezius muscle; cervid = right sternocleidomastoid muscle; cervie = left sternocleidomastoid muscle.
Fig. 1First session of masticatory muscles clenching
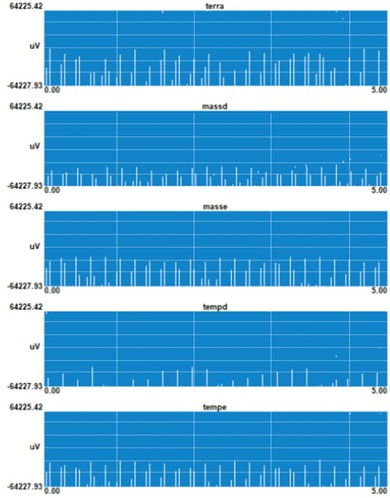
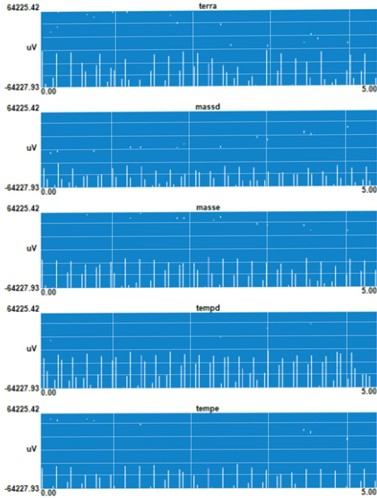
Fig. 2Second session of masticatory muscles clenching
The image shows the first electromyographic recording of the maximum intercuspation of the masticatory muscles. The ground wire served as a reference for analysis of the electromyographic activity. Results: Right Masseter presented low electrical activity; Left Masseter with greater electrical activity; Right Temporal with electrical activity well below the expected. Left Temporal with electrical activity higher than the right temporal muscle. This image was disregarded due to discrepancy with the images in Fig. 2 and Fig. 3.
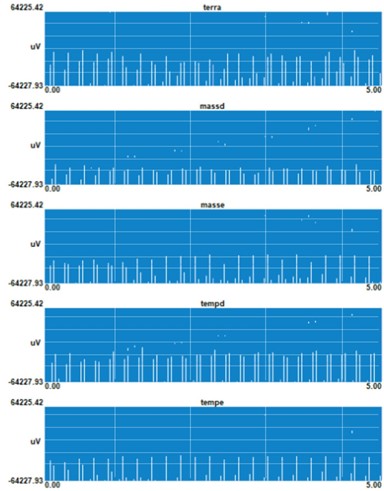
In the second and third sessions, there was a significant increase in the electrical activity of the right temporal, but the left masseter remained with greater activity in relation to the right masseter. As the electrical activities of both sessions demonstrated equivalence, it was considered that the right temporal presented greater electromyographic activity than the left temporal. The left masseter presented greater muscle activity in the second and third sessions, the right masseter presented low electrical activity (Fig. 2), (Fig. 3).
Fig. 2 results: The right masseter presented a much lower electrical activity compared to the ground wire; Left masseter with greater electrical activity compared with the right masseter; Right temporal with a significant increase compared to fig1 presenting a high electrical activity; Left temporal with a low electrical activity.
Fig. 3Third Session masticatory muscles clenching

Fig. 4First resting session of the masticatory muscles

Fig. 3 results: The right masseter had lower electrical activity compared with the left masseter; the left masseter had a higher electrical activity close to normal; the right temporal muscle showed high electrical activity; and the left temporal muscle showed low muscular activity compared to the ground wire
During rest, the masticatory muscles showed different results. The right masseter showed lower muscular activity compared with the left masseter (Fig. 4). The left masseter and right temporal muscles showed an increase in electrical activity in the second and third sessions compared to the first session, in contrast to the right masseter and left temporal muscles, which showed lower electrical activity in the last two sessions compared to the first.
Fig. 4 results: During rest, the right masseter presented lower electrical activity than the left masseter during the resting condition.; the left masseter presented high muscle activity even when at rest; the right temporal muscle presented high muscle activity; the left temporal muscle presented electrical activity close to that of a muscle at rest.
Fig. 5 results: The right masseter presented electrical muscle activity close to rest; the left masseter, right temporal muscle, left temporal muscle presented electrical muscle activity that did not correspond to rest, with greater activity in the right temporal muscle.
Fig. 6 results: The right masseter presented electrical muscle activity close to resting; Left masseter, right temporal, left temporal presented electrical muscle activity that did not correspond to the resting.
Fig. 5Second resting session of the masticatory muscles

Fig. 6Third resting session of the masticatory muscles
The recording of the electrical activity of the cervical muscles during maximum intercuspation resulted in the right sternocleidomastoid muscle having a higher electrical activity, as well as the right trapezius muscle; this pattern was maintained in the three sessions (Figs. 7-9).
Fig. 7First session of cervical and trapezius muscles clenching

Fig. 8Second session of cervical and trapezius muscles clenching

Fig. 9Third session of cervical and trapezius muscles clenching
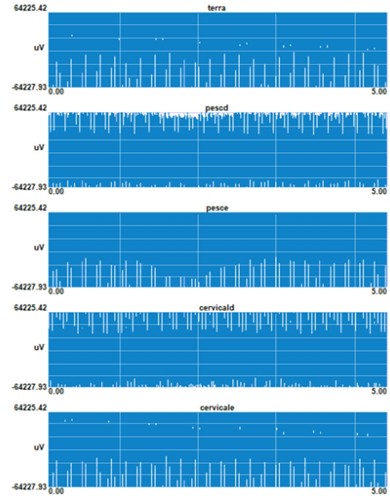
Fig. 10First resting session of cervical and trapezius muscles
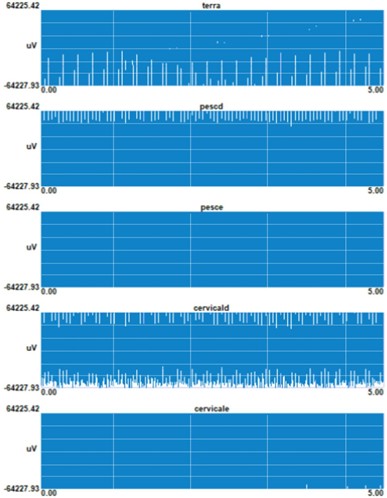
Fig. 11Second resting session of cervical and trapezius muscles
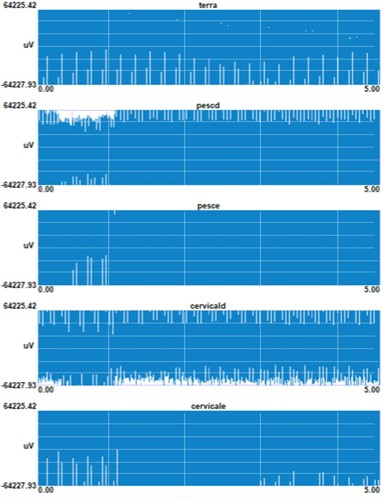
Fig. 12Third resting session of cervical and trapezius muscles
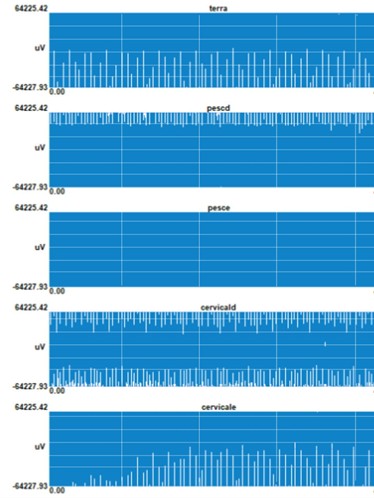
Fig. 7 results: The right sternocleidomastoid muscle with a greater electrical activity than the left sternocleidomastoid muscle; Right trapezius muscle with a greater muscular activity in relation to the left trapezius muscle.
Fig. 8 results: The right sternocleidomastoid muscle with a greater electrical activity than the left sternocleidomastoid muscle; Right trapezius muscle with a greater muscular activity in relation to the left trapezius muscle.
Fig. 9 results: The right sternocleidomastoid muscle with a greater electrical activity than the left sternocleidomastoid muscle; Right trapezius muscle with a greater muscular activity in relation to the left trapezius muscle.
At rest, the right sternocleidomastoid muscle and the right trapezius showed increased muscle activity, while the corresponding muscles on the left side showed muscle activity closer to the ideal when the musculature is at rest (Figs. 7-9).
Fig. 10 results: The right sternocleidomastoid muscle had a different high electrical activity than the left sternocleidomastoid muscle, which was at rest. The right trapezius had a different high electrical activity than the left trapezius, which was at rest.
Fig. 11 results: The right sternocleidomastoid muscle had a high electrical activity different from the left sternocleidomastoid muscle which was at rest. The right trapezius had a high electrical activity different from the left trapezius which was at rest.
Fig. 12 results: The right sternocleidomastoid muscle had a high electrical activity different from the left sternocleidomastoid muscle which was at rest. The right trapezius had a high electrical activity different from the left trapezius which was at rest.
3. Discussion
This case report aimed to observe the muscle behaviour in maximum intercuspation and at rest, focusing on the masticatory and neck muscles. Specifically, the results indicated that: (1) the left masseter and right temporal muscles showed greater electrical activity in MHI, (2) at rest, with the exception of the right masseter, all masticatory muscles showed muscle activity, (3) the right sternocleidomastoid and right trapezius in MHI presented elevated ECG, (4) at rest this pattern was repeated with electrical activity of the right sternocleidomastoid and right trapezius. Bilateral volume, bilateral jump, left-sided popping, pain on the left side forced movement, pain on left side passive movement, pain on the left side masseter and right temporal, left-sided and right-sided temporal pain on palpation, limited movement. Trapezius, lumbar, and behind-the-knee pain.
The body is a system that works according to the principle of compensation when a disturbance occurs, such as muscle tension. This will cause compensatory changes in muscle tension in the spinal column region, forcing a more correct posture, within the body’s tolerance [16].
When this compensation exceeds the individual's threshold, symptoms such as pain may occur. Studies by Huggare and Sonnensen indicate a relationship between cervical pain as a result of compensation caused by temporomandibular dysfunction (TMD) [17], [18]. This relationship may be associated with biomechanical, neuroanatomical and neurophysiological factors, in addition to muscular disorders mainly between the masticatory muscles and the cervical muscles [19].
Incorrect tension in the masticatory muscles may be associated with head posture, suggesting one of the causes of cervical muscle dysfunctions [20]. Despite the relationship between TMD and the presence of pain, a study by Ries demonstrated that approximately 43 % of the individuals in the study did not present cervical pain [21]. Meanwhile the study by Li J observed the electromyography (EMG) of the masseter and temporal muscles in cases of orofacial pain, concluding that the group with pain had an increase in EMG activity at rest, in addition, patients who 15 presented bilateral pain presented greater electrical activity compared to the group with unilateral pain [22].
An asymmetric relationship of electrical activity during mastication was found in patients with TMD. The temporal, masseter and sternocleidomastoid muscles showed abnormal activity. This asymmetry was interpreted as a way to compensate for the mandible and cervical region stability during mastication [21], [23].
Pain is related to greater electrical activity in the muscles of the neck region when compared to people without pain, which indicates a control pattern for compensation and protection for the muscles with painful symptoms [24]. The muscles affected by an irregular head posture are: masseter and trapezius, increasing the chance of developing TMD or vice versa [25], [26]. In addition, one of the consequences for the masticatory muscle would be fatigue, which could be the result of TMD or a cervical muscular dysfunction [26].
Body compensation for an imbalance, whether it is cervical, occlusal or due to TMD, can have effects on posture, resulting in changes such as: femur size, cervical lordosis or even scoliosis [25]. A study with 50 patients aged 12 to 18 years old with idiopathic scoliosis and 50 healthy patients, demonstrated a relationship between TMD and scoliosis. The group with scoliosis demonstrated a higher incidence of TMD compared to the healthy group. The study concluded a possible relationship, as well as demonstrating painful symptoms in the lumbar region [26].
Other studies have shown a relationship between temporomandibular dysfunction and postural changes such as cervical lordosis, which is related to mandibular deviation. Changes in posture can lead to adaptations in the position of the head, neck muscles, masticatory muscles, ligaments and temporomandibular joint. When this adaptation exceeds the patient’s threshold, pain may appear [25], [26]. Contrary to what has been reported, Manfredini reports in his study that temporomandibular dysfunction does not have the ability to alter body position [26].
This study has some limitations. First, it is a clinical case report that, despite providing information on the muscle function of the neck region and the temporomandibular joint region during MIH and during rest, presents a single individual. This study in a larger scale may outcome in different results. Second, although a second electromyographic recording was performed 15 minutes after the initial assessment, it was not possible to perform a long-term follow-up evaluation after a therapeutic intervention. Future studies should include post-treatment assessments to better understand the relationship between muscle disorders and temporomandibular dysfunction.
4. Conclusions
In conclusion, electromyographic alterations are related to patients with temporomandibular dysfunction, explaining the alterations in the clinical examination of the temporomandibular joint, such as: bilateral volume of the masseter and temporal muscles, pain on palpation of the masseter and temporal muscles, nodules in the masseter, pain in passive and forced movement in the masseter and temporal muscles, and movement limitation. These alterations can trigger changes in cervical posture that could explain the pain in the sternocleidomastoid, trapezius, lumbar muscles, and pain in the popliteal region. However, further investigations with a larger number of individuals are necessary to confirm such relationships, in addition to performing treatment to evaluate the muscular response.
References
-
Y.-T. Jou, “Dental deafferentation and brain damage: A review and a hypothesis,” The Kaohsiung Journal of Medical Sciences, Vol. 34, No. 4, pp. 231–237, 2018, https://doi.org/10.1016/j.kjms.2018.01.013
-
L. Guarda-Nardini, A. Stecco, C. Stecco, S. Masiero, and D. Manfredini, “Myofascial pain of the jaw muscles: Comparison of short-term effectiveness of botulinum toxin injections and fascial manipulation technique,” Cranio, Vol. 30, No. 2, pp. 95–102, 2012, https://doi.org/10.1179/crn.2012.014
-
R. Kielnar et al., “The influence of cervical spine rehabilitation on bioelectrical activity (sEMG) of cervical and masticatory system muscles,” Plos One, Vol. 16, No. 4, p. e0250746, Apr. 2021, https://doi.org/10.1371/journal.pone.0250746
-
S. Silva Ulloa, A. L. Cordero Ordóñez, and V. E. Barzallo Sardi, “Relationship between dental occlusion and brain activity: A narrative review,” The Saudi Dental Journal, Vol. 34, No. 7, pp. 538–543, 2022, https://doi.org/10.1016/j.sdentj.2022.09.001
-
M. G. Piancino, A. Tortarolo, A. Polimeni, E. Bramanti, and P. Bramanti, “Altered mastication adversely impacts morpho-functional features of the hippocampus: A systematic review on animal studies in three different experimental conditions involving the masticatory function,” Plos One, Vol. 15, No. 8, p. e0237872, 2020, https://doi.org/10.1371/journal.pone.0237872
-
A. Quintero, E. Ichesco, C. Myers, R. Schutt, and G. E. Gerstner, “Brain activity and human unilateral chewing,” Journal of Dental Research, Vol. 92, No. 2, pp. 136–142, 2012, https://doi.org/10.1177/0022034512466265
-
J. H. Kim, J. K. Oh, J. H. Wee, Y. H. Kim, S.-H. Byun, and H. G. Choi, “Association between tooth loss and Alzheimer’s disease in a nested case-control study based on a national health screening cohort,” Journal of Clinical Medicine, Vol. 10, No. 17, p. 3763, 2021, https://doi.org/10.3390/jcm10173763
-
Y. Matsuka, “Orofacial pain: Molecular mechanisms, diagnosis, and treatment 2021,” International Journal of Molecular Sciences, Vol. 23, No. 9, p. 4826, 2022, https://doi.org/10.3390/ijms23094826
-
K. Randow, K. Carlsson, J. Edlund, and T. Oberg, “The effect of an occlusal interference on the masticatory system,” Odontologisk Revy, Vol. 27, pp. 245–256, 1976.
-
M. Kalladka, A. Young, D. Thomas, G. M. Heir, S. Y. P. Quek, and J. Khan, “The relation of temporomandibular disorders and dental occlusion: a narrative review,” Quintessence International, Vol. 53, No. 5, pp. 450–459, 2022, https://doi.org/10.3290/j.qi.b2793201
-
R. Ciancaglini, E. F. Gherlone, and G. Radaelli, “Association between loss of occlusal support and symptoms of functional disturbances of the masticatory system,” Journal of Oral Rehabilitation, Vol. 26, No. 3, pp. 248–253, Dec. 2001, https://doi.org/10.1046/j.1365-2842.1999.00368.x
-
V. F. Ferrario, C. Sforza, and G. Serrao, “The influence of crossbite on the coordinated electromyographic activity of human masticatory muscles during mastication,” Journal of Oral Rehabilitation, Vol. 26, No. 7, pp. 575–581, Dec. 2001, https://doi.org/10.1046/j.1365-2842.1999.00419.x
-
C. Riise and A. Sheikholeslam, “Influence of experimental interfering occlusal contacts on the activity of the anterior temporal and masseter muscles during mastication,” Journal of Oral Rehabilitation, Vol. 11, No. 4, pp. 325–333, Jun. 2007, https://doi.org/10.1111/j.1365-2842.1984.tb00583.x
-
L. Germain, “Differential diagnosis of toothache pain: Part 2, nonodontogenic etiologies,” Dentistry Today, Vol. 31, No. 8, pp. 88–89, 2012.
-
J. Huggare, A. M. Raustia, and H. W. Makofsky, “Head posture and cervicovertebral and craniofacial morphology in patients with craniomandibular dysfunction,” Cranio, Vol. 10, No. 3, pp. 173–179, 2016, https://doi.org/10.1080/08869634.1992.11677908
-
L. Sonnesen, “Temporomandibular disorders in relation to craniofacial dimensions, head posture and bite force in children selected for orthodontic treatment,” The European Journal of Orthodontics, Vol. 23, No. 2, pp. 179–192, 2001, https://doi.org/10.1093/ejo/23.2.179
-
M. Ghodrati et al., “Adding temporomandibular joint treatments to routine physiotherapy for patients with non-specific chronic neck pain: A randomized clinical study,” Journal of Bodywork and Movement Therapies, Vol. 24, No. 2, pp. 202–212, Apr. 2020, https://doi.org/10.1016/j.jbmt.2019.11.004
-
B. Häggman-Henrikson, E. Lampa, S. Marklund, and A. Wänman, “Pain and disability in the jaw and neck region following whiplash trauma,” Journal of Dental Research, Vol. 95, No. 10, pp. 1155–1160, Jul. 2016, https://doi.org/10.1177/0022034516653598
-
L. G. K. Ries et al., “Influence of craniomandibular and cervical pain on the activity of masticatory muscles in individuals with temporomandibular disorder,” CoDAS, Vol. 26, No. 5, pp. 389–394, Oct. 2014, https://doi.org/10.1590/2317-1782/20142014040
-
J. Li, T. Jiang, H. Feng, K. Wang, Z. Zhang, and T. Ishikawa, “The electromyographic activity of masseter and anterior temporalis during orofacial symptoms induced by experimental occlusal highspot,” Journal of Oral Rehabilitation, Vol. 35, No. 2, pp. 79–87, Jan. 2008, https://doi.org/10.1111/j.1365-2842.2007.01750.x
-
C. M. de Felício, A. Mapelli, F. V. Sidequersky, G. M. Tartaglia, and C. Sforza, “Mandibular kinematics and masticatory muscles EMG in patients with short lasting TMD of mild-moderate severity,” Journal of Electromyography and Kinesiology, Vol. 23, No. 3, pp. 627–633, Jun. 2013, https://doi.org/10.1016/j.jelekin.2013.01.016
-
S. O. ’Leary, D. Falla, and G. Jull, “The relationship between superficial muscle activity during the cranio-cervical flexion test and clinical features in patients with chronic neck pain,” Manual Therapy, Vol. 16, No. 5, pp. 452–455, Oct. 2011, https://doi.org/10.1016/j.math.2011.02.008
-
D. T. Shewman and B. A. Kin, Surface Electromyography in Temporomandibular Dysfunction: a Beginner’s Guide to Clinical Applications. Indianapolis, IN, USA: BioResearch Associates, 2006.
-
I. Uçar et al., “Is scoliosis related to mastication muscle asymmetry and temporomandibular disorders? A cross-sectional study,” Musculoskeletal Science and Practice, Vol. 58, p. 102533, Apr. 2022, https://doi.org/10.1016/j.msksp.2022.102533
-
K.-C. Lee, Y.-T. Wu, W.-C. Chien, C.-H. Chung, L.-C. Chen, and Y.-S. Shieh, “The prevalence of first-onset temporomandibular disorder in low back pain and associated risk factors,” Medicine, Vol. 99, No. 3, p. e18686, 2020, https://doi.org/10.1097/md.0000000000018686
-
M. Yelken Kendirci, A. F. Ertürk, I. Özcan, A. Kendirci, and T. Akgül, “The role of scoliosis on temporomandibular joint disease: A cross-sectional study based on ultrasonography,” Clinical Radiology, Vol. 79, No. 3, pp. e417–e423, Mar. 2024, https://doi.org/10.1016/j.crad.2023.11.023
About this article

The authors have not disclosed any funding.
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Vitoria Peixoto: conceptualization ideas, data curation, formal analysis, investigation, methodology, project administration, supervision, visualization, writing- original draft preparation, writing- review and editing preparation. Maíra Barroso: formal analysis, validation, visualization, writing- review and editing preparation. Janaína Nunes: formal analysis, validation, visualization, review and editing preparation. Orlando Santiago: conceptualization ideas, data curation, methodology, supervision, writing- review and editing preparation.
Prof. Orlando Santiago Júnior is an editor in chief for Jaw Functional Orthopedics and Craniofacial Growth and was not involved in the editorial review and/or the decision to publish this article.
Its a case report, in this case ethics statement was not necessary.
